Navigating AHPRA’s New Aesthetic Guidelines: A Clinical Masterclass
- Mike D Clague

- Jun 15
- 5 min read
In the rapidly evolving landscape of Australian aesthetic medicine, 2026 marks a definitive shift. The "wild west" era of cosmetic injectables is being systematically dismantled by the Australian Health Practitioner Regulation Agency (AHPRA) and the Medical Board of Australia (MBA).
For many, these guidelines: focused on psychological screening, mandatory cooling-off periods, and stricter supervision: feel like a bureaucratic hurdle.
However, for the elite practitioner, these regulations are a welcome formalisation of what we have always championed: clinical mastery as the ultimate form of patient safety.
As a practitioner with over 23 years of experience and 40,000 treatments performed, I’ve seen trends come and go. I’ve seen the rise of "social media injectors" and the subsequent fallout of complications.
My philosophy has always been rooted in radical evidence-based medicine. Whether I am lecturing at Monash University or treating patients in my clinics in Auckland, Queenstown, Melbourne and Sydney, my message remains the same: If you prioritize the architecture of the face and the biology of the tissue, compliance isn't a chore: it’s a byproduct of excellence.
Compliance Through Clinical Mastery: Why Safety is Your Best Legal Protection
The new AHPRA guidelines emphasize that practitioners must work only within their competence and scope. This sounds simple, but in a field where three-day "masterclasses" are sold as comprehensive training, "competence" is often overestimated.
True competence isn't just knowing where to poke a needle; it’s understanding the rheology of the product, the anatomical variations of the facial arteries, and the psychological profile of the patient in front of you.
AHPRA now mandates screening for Body Dysmorphic Disorder (BDD). To the unseasoned injector, this is a box to tick. To a clinical mentor, this is a diagnostic imperative.
The best practitioners know how to say NO.
Refusing treatment to a patient who does not meet the psychological or anatomical criteria for a safe, natural result is not a loss of revenue: it is the protection of your professional integrity.
In my own practice, I may choose not to treat you if the goals don't align with the structural needs of your face. This level of transparency is what the new guidelines are striving for, and it is what I teach in my professional clinical training courses.
The Gold Standard for Emergencies: The Supra-Orbital Notch Technique
One of the most significant contributions I’ve made to this industry: alongside my colleague Dr. Greg Goodman: was the documentation of the first successful reversal of HA filler-induced blindness. Our 2016 paper, "A rethink on hyaluronidase injection," changed the management algorithm for ocular emergencies.

While many older protocols suggested high-risk retrobulbar injections, our research pointed to a safer, more effective "Gold Standard": flooding the supra-orbital notch (targeting the supra-orbital and supratrochlear foramen) with high-dose hyaluronidase.
The rationale is architectural and biological: these vessels are branches of the ophthalmic artery. By delivery of the enzyme at these exit points, we can retrograde the hyaluronidase to dissolve the embolus.

When you understand the anatomy at this level, you aren't just "injecting"; you are performing a medical intervention with a profound understanding of risk mitigation. This is the difference between a "tweakment" and medical aesthetics.
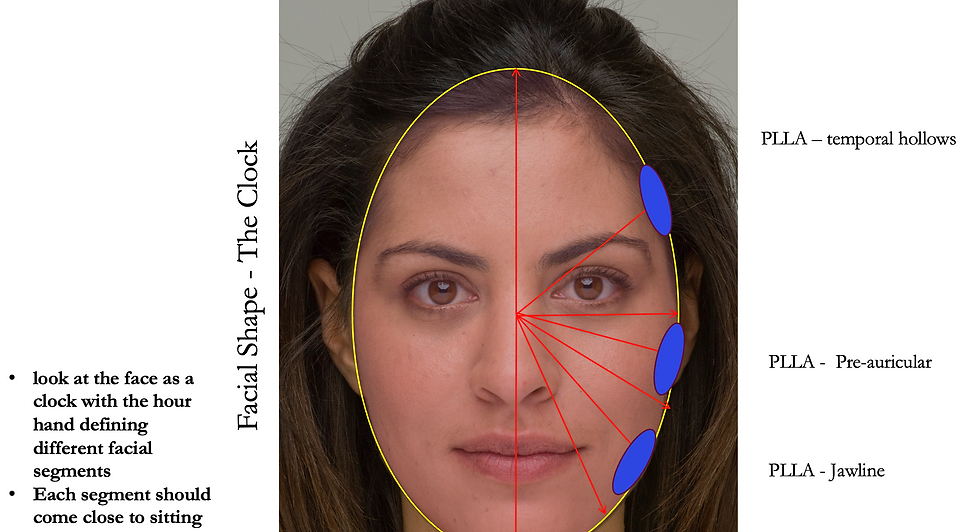
The Assessment Philosophy: Outside-In and "LIPS GO LAST"
A common mistake I see among less experienced injectors: often fueled by patient demand and Instagram trends: is treating the face as a collection of isolated parts. A patient asks for lips, and the injector fills the lips. This is fundamentally flawed.
In my clinic, we follow a strict 'outside-in, top-to-bottom' assessment philosophy. We look at the scaffolding first. If the mid-face has lost volume, or the temples have hollowed, filling the lips will only create an unbalanced, "done" look that lacks harmony.
The Protocol:
Deep Restoration: We start with the foundation. This often involves Sculptra biostimulators to activate fibroblasts and restore the skin's natural "scaffolding" over time.
Structural Support: Addressing the lateral face and malar fat pads to lift and support.
Refinement: Only once the architecture is restored do we look at the central features.
LIPS GO LAST: The mouth is the finishing touch. If you do it first, you lose the map of the face.
This sequencing ensures that the result is "undone": a refreshed, natural look that respects the original architecture of the patient's face.

The "Patreon Slant": Your Clinical Mentor in Your Pocket
The shift in Australian regulations means that the era of "learning on the fly" is over. Doctors and nurses now require documented evidence of ongoing clinical mentorship and evidence-based education.
Social media is a terrible place to learn medicine. It prioritizes the "before and after" over the "how and why." It glamorizes procedures that, frankly, lack rigorous scientific backing. I am vocally skeptical of trends like Rejuran or "snatched" jawlines that prioritize marketing hype over peer-reviewed data.
This is why I built my Patreon for Cosmetic Injectors.
It is designed to be a "clinical mentor in your pocket." We move away from the marketing fluff and dive into deep technical analysis, technical videos, and the latest published research. For the medical professional who wants to master the supra-orbital notch technique or understand the nuances of PLLA vs. PDLLA biostimulators, this platform provides the "high brow" clinical language and technical depth that AHPRA standards now demand.
Join the Patreon community here to access over 23 years of clinical expertise.
Radical Honesty in a Regulated Era
AHPRA’s new rules on advertising: banning testimonials and restricting how we use "before and after" photos: are designed to prevent the trivialisation of medical procedures. I welcome this.
We should not be selling "beauty"; we should be providing medical services. This requires radical honesty.
Don't lie about the longevity of a product.
Don't downplay the risks of vascular occlusion.
Do explain the biological process of collagen stimulation.
When you speak to a patient with the authority of an educator, they don't just feel "sold" to: they feel cared for. Whether you are a nurse injector starting your journey or a seasoned doctor looking to refine your emergency protocols, the goal is the same: clinical mastery.
Conclusion: The Future of Australian Aesthetics
The 2026 landscape in Australia is not a threat to our industry; it is a filter. It will filter out those who are here for the trend and leave behind the professionals who are here for the patients.
By adhering to a "safety-first" mindset, utilizing evidence-based techniques like the supra-orbital notch approach, and following a logical "outside-in" assessment, you aren't just complying with AHPRA: you are leading the industry.
For those ready to commit to this level of mastery, I invite you to join me in the clinic or via my global mentorship platform. Let’s move past the "tweakment" and back into the realm of architectural, biological restoration.
Mike Clague (NMW0001618803) is an Adjunct Lecturer at Monash University and a global educator in medical aesthetics. He consults in Auckland, Melbourne and Sydney and provides elite training for medical professionals worldwide.
Comments